



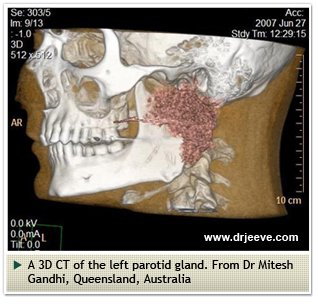
The salivary glands are situated in the head and neck and are important organs. They produce between 0.5 – 1.5 litres of saliva a day. Saliva has an important role in the preparation of food for digestion by the stomach, and in the lubrication of the mouth, pharynx and voice box. There are three paired major salivary glands – the parotid glands in front of the ears, the submandibular glands below in jaw and the sublingual glands in the floor of the mouth. There are also hundreds of smaller 'minor' salivary glands in the lining of the mouth and throat that produce saliva.
There are many diseases that affect the salivary glands.These include:
Salivary gland infections or sialadenitis are common. The most common infection of the salivary gland is mumps caused by a paramyxovirus. With vaccination, this is rarely seen. We tend to see bacterial infections of the salivary glands these days. The source of these bacteria is the mouth. Hence, poor dentition and dental plaque tend to be predisposing factors.
Some patients have a damaged salivary gland duct that tends to predispose them to slow-flowing saliva. This salivary ‘stasis’ can lead to a build-up of ‘sludge’ and an infection. Infections are more common in those who do not hydrate well and in the elderly. Some infections may develop into abscesses that require drainage. Most infections are self-limiting and resolve well with antibiotics.
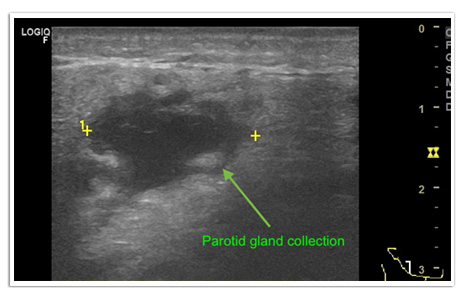
I routinely use ultrasound to monitor infections closely. In this patient a collection developed that responded well to needle aspiration under ultrasound guidance
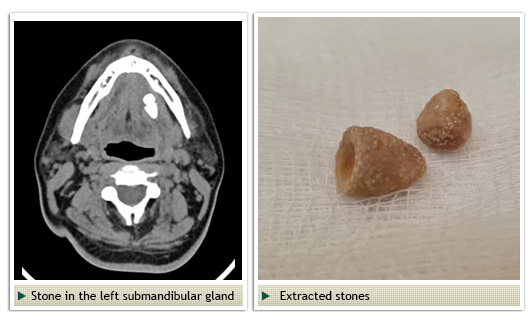
Salivary gland stones are common in the submandibular salivary gland and parotid salivary gland. These stones may vary in size from a 2-3 mm to over 2 cms. The stones obstruct the flow of saliva and cause the saliary gland to swell. This leads to discomfort and pain. Typically, eating which stimulates salivary flow leads to swelling.
Small stones may extrude spontaneously. If they do not, extraction may be necessary. Conventionally, an incision is made into the ductal opening (papilla) to allow the stone to be passed. In recent years, stones can be removed with sialendoscopy which utilizes fine scopes to examine the ducts of these glands and remove any stones.

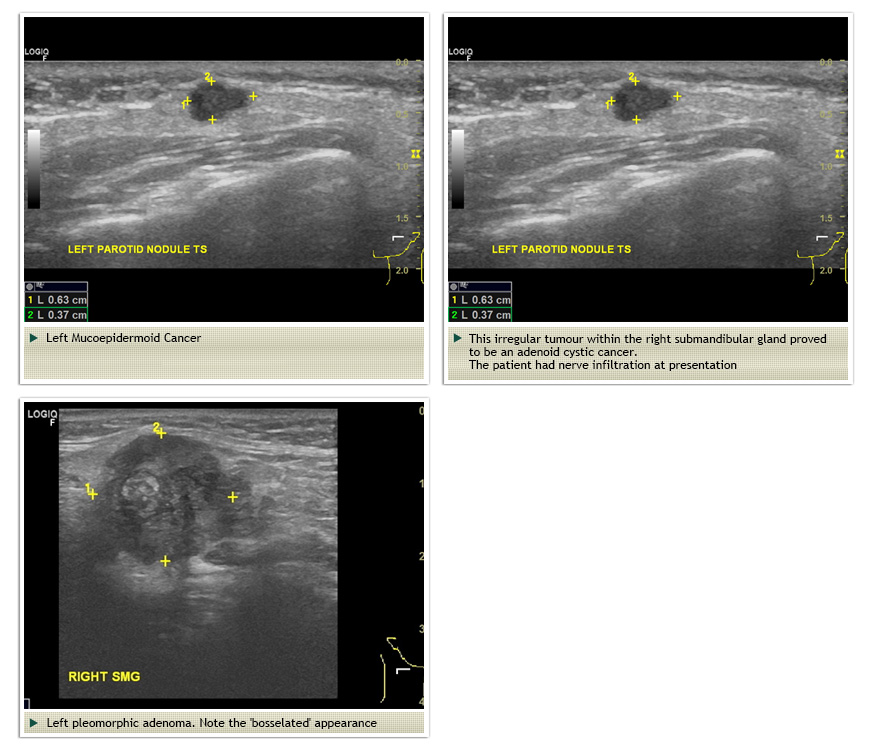
Tumours or masses within the salivary glands may be benign or malignant. Eighty percent of parotid tumours are benign whereas only 60% of submandibular gland tumours and a small percentage of minor salivary gland tumours are benign. There are more than 20 varieties of salivary gland cancers – the most common variety is a mucoepidermoid carcinoma which maybe low, intermediate or high grade. Salivary gland cancers usually present as painless lumps in the neck. Mucoepidermoid cancers may occasionally be painful so the dictum that painful lumps are less likely to be malignant does not apply.
Adenoid cystic salivary cancers tend to be aggressive cancers. They have a tendency to infiltrate and spread along nerves. These patients may present with weakness of the facial muscles that are innervated by branches of the facial nerve which pass close to the submandibular and parotid salivary glands.
The most common benign salivary gland tumour is a pleomorphic adenoma. Although benign, these have a tendency to recur after surgical removal. It is important that surgery for pleomorphic adenomas is performed well to ensure complete removal and no tumour spillage during extirpation.
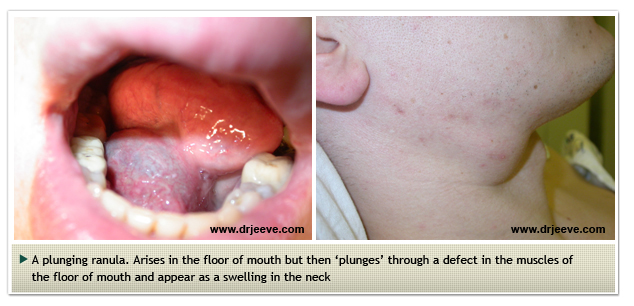
Cysts may arise from the ducts of salivary glands. The picture below is of a cyst called a plunging ranula. There is evidence of a cyst in the floor of mouth as well as protrusion of this cyst into the neck.
Surgery to remove the salivary glands is often necessary when a tumour is present or in the presence of a large stone deep within the gland. Some benign tumours such as pleomorphic adenomas have a propensity to turn malignant and therefore requires surgical removal too.
The common operations are:
The following video demonstrates the branches of the facial nerve which have been dissected out following a superficial parotidectomy
